Plaque, Atherosclerosis & Silent Heart Disease: What You Cannot Feel Can Still Kill You
Dr. Peter Chang
Triple Board-Certified Cardiologist & Vascular Specialist
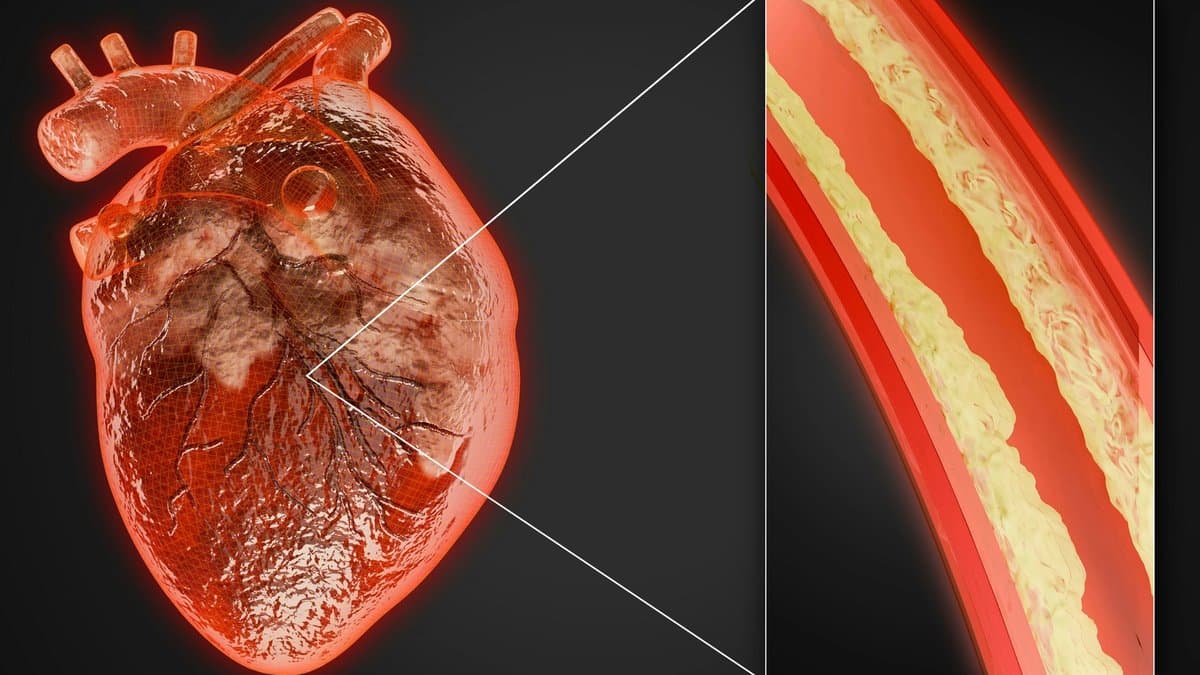
What Is Atherosclerosis?
Why the First Symptom Is Often a Heart Attack
Who Is at Risk of Silent Atherosclerosis?
- Elevated LDL cholesterol — the primary initiator of plaque formation and expansion
- Hypertension — accelerates endothelial injury
- Diabetes and insulin resistance — trigger inflammation and accelerate plaque development
- Smoking — directly damages the endothelium and promotes clotting
- Family history of premature coronary disease — a close relative with heart attack or coronary procedure before age 55 (men) or 65 (women)
- Elevated Lp(a) — a genetically determined risk factor present in ~20% of the population, absent from routine cholesterol panels
Detecting Plaque Before a Heart Attack
CT Coronary Angiography and Other Tools
What You Can Do
When to Seek Assessment
Frequently Asked Questions
Common Questions About Plaque, Atherosclerosis & Silent Heart Disease
Can you have serious heart disease without any symptoms?
Yes — this is the defining feature of atherosclerosis. The artery remodels outward as plaque accumulates, preserving normal blood flow until the disease is advanced. Up to 50% of first heart attacks occur in people with no prior symptoms, no known heart disease, and no abnormal stress test.
What is the best test to detect silent heart disease in Singapore?
Coronary Artery Calcium (CAC) scoring is the most validated, cost-effective screening tool for asymptomatic individuals. For those with symptoms or equivocal findings, CT Coronary Angiography (CTCA) provides more detailed anatomical information including non-calcified plaque.
Can atherosclerosis be reversed?
Established calcified plaque cannot be dissolved. However, statin therapy stabilises plaque, thickens the fibrous cap, shrinks the lipid core, and substantially reduces the risk of rupture. With intensive risk factor management, progression can be significantly slowed and in some cases halted.
What is Lp(a) and why does it matter?
Lipoprotein(a) is a genetically determined cardiovascular risk factor that is not measured in a standard cholesterol panel. It is elevated in approximately 20% of the population and substantially increases both plaque burden and the risk of plaque rupture. Everyone with premature heart disease, a strong family history, or unexplained high CAC should be tested for Lp(a) at least once.
At what age should I start screening for heart disease in Singapore?
For individuals with risk factors (family history, diabetes, hypertension, smoking, elevated cholesterol), cardiovascular screening should begin by age 40. For those with a strong family history of premature coronary disease, screening as early as 35 may be appropriate. Your cardiologist will recommend the most suitable screening strategy based on your individual profile.